What would good quality assurance look like in primary care?
- Primary care
- Lived experience
- Person-centred care
- Integrated care
- Communication and administration
About the Quality and Outcomes Framework (QOF)
In 2018, when the Quality and Outcomes Framework (QOF) was last under review, many of our members voiced their concerns about the potential loss of QOF. While QOF plays an important role in incentivising quality patient care, it also generates important data on the state of patient care across conditions and communities in England.
In May 2023, the Government published its Primary Care Recovery Plan and committed to consult on the future of QOF and the Investment and Impact Fund (IIF). IIF is an incentive scheme focused on supporting primary care networks (PCNs) to deliver high quality care to their population, and the delivery of the priority objectives articulated in the NHS Long Term Plan and in Investment and Evolution.
Our work on QOF
In November 2023, we held a roundtable session with members and people with lived experience to gain a clear picture of the perspectives of diverse groups of patients and patient charities on the future of financial incentives and quality assurance within primary care.
Our report, What would good quality assurance look like in primary care, is the result of this discussion. In addition to presenting the insights from this discussion, from a range of both community and condition focused charities, it identifies key issues and priority actions for strengthening quality assurance of primary care.
Our recommendations
Our report urges the consultation to form just the first engagement of a QOF review. The Voluntary, Community and Social Enterprise sector and people with lived experience are able to add vital support around operational changes such as qualitative measurement, communication needs and a refocus on health inequalities.
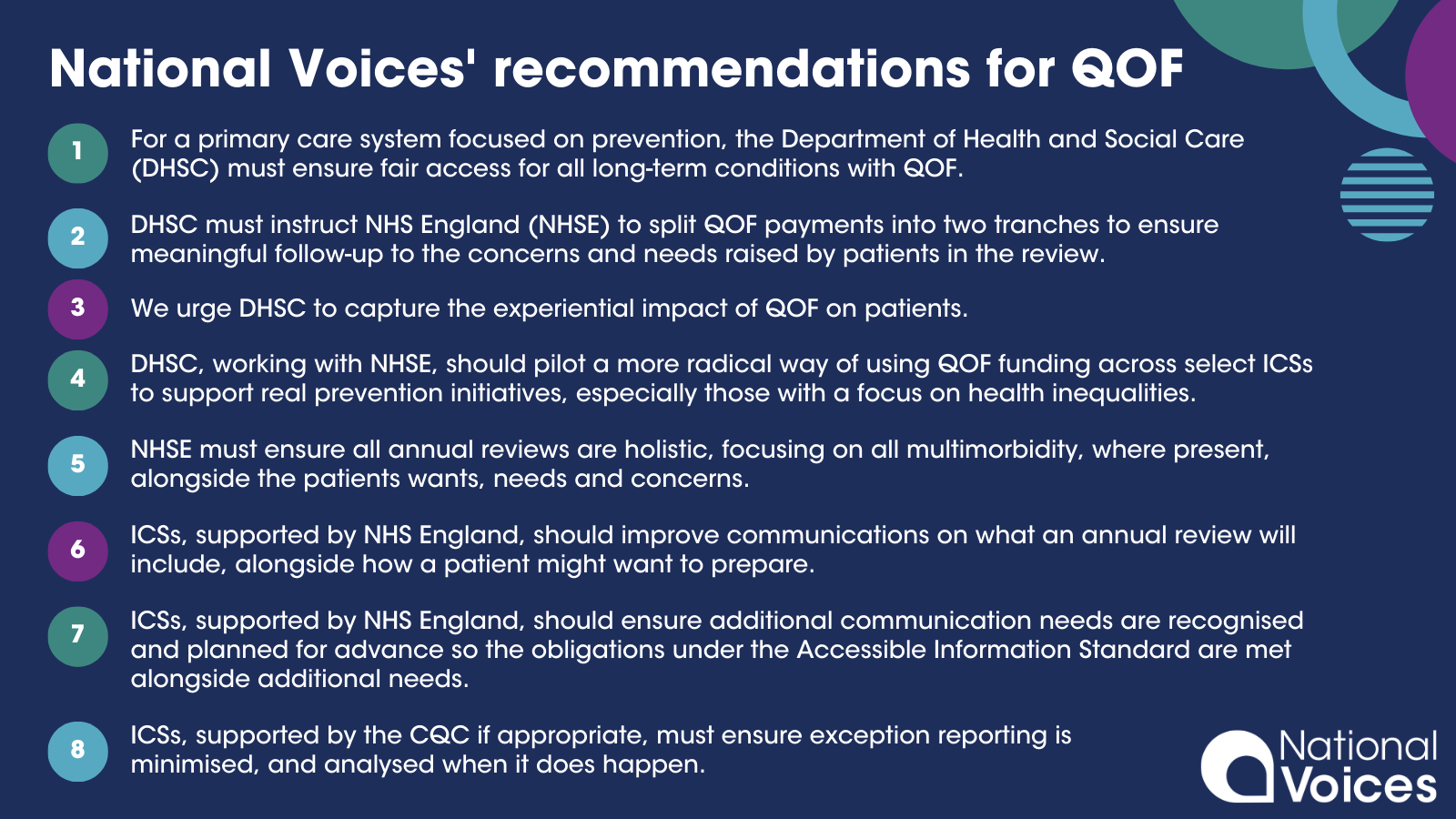
With that said we have developed eight clear recommendations:
- For a primary care system focused on prevention, the Department of Health and Social Care (DHSC) must ensure fair access for all long-term conditions with QOF enabling everyone with a long-term health condition to receive a high-quality annual review.
- DHSC must instruct NHS England to split QOF payments into two tranches to ensure meaningful follow-up to the concerns and needs raised by patients in the review, whether this be additional diagnosis and treatment, or support to better self-manage.
- We urge DHSC to capture the experiential impact of QOF on patients. As it currently stands, QOF financial payments focus on quantitative measures which do not reflect the value that QOF is intended to offer to patients.
- DHSC, working with NHS England, should pilot a more radical way of using QOF funding across select ICSs to support real prevention initiatives, especially those with a focus on health inequalities. This pilot should also include how to reutilise alternative data sets to ensure quality improvement is maintained.
- To ensure patient trust and their ability to self-manage are maximised, NHS England must ensure all annual reviews are holistic, focusing on all multimorbidity, where present alongside the patients wants, needs and concerns.
- Integrated Care Systems (ICSs), supported by NHS England, should improve communications on what an annual review will include, alongside how a patient might want to prepare. This will ensure people accessing primary care are empowered to access care and support in a way that works best for them and understand the full support offer available to them.
- ICSs, supported by NHS England, should ensure additional communication needs are recognised and planned for advance so the obligations under the Accessible Information Standard are met alongside additional needs such as translators.
- ICSs, supported by the CQC if appropriate, must ensure exception reporting is minimised, and analysed when it does happen, to ensure bad practice is weeded out and community need is identified.
We have created a shareable graphic, presenting these eight recommendations, which you are free to use.
{kind=link}
If you would like to read this report in an alternative format, please get in touch.
Acknowledgements
We would particularly like to thank our member organisations and people with lived experience of accessing primary care services for sharing their insights and inputting on this work, including Allergy UK, Aspergillosis Trust, Asthma+Lung UK, British Heart Foundation, Diabetes UK, Dementia UK, Epilepsy Action, Pancreatic Cancer UK, Prostate Cancer UK, Rethink Mental Illness, South Asian Health Action, Versus Arthritis, and others.
We would also like to thank our Partners, including the King’s Fund and Nuffield Trust, and others for their input and advice on this independent report.
AstraZeneca has provided a sponsorship grant towards this independent programme.